By Iris Farrou
17 Oct, 2023
Childhood Health, Fatherhood, New Moms, Prevention, Procedures, Toddler Health, Your baby's health
allergic to, Allergy to medicine, antihistamines safe for babies, asthma, Baby Allergies, Blood test for babies, cats, dogs, dust, dust allergy, exzema, food sensitivity, How do I know if my baby has allergies, how to diagnose, Infant, is allergic, mold, Pediatric Allergist, Pediatrician, pets, toddlers, What age is safe for allergen exposure, what are the symptoms of anaphylactic shock
 We all know babies are fragile, and none other than parents of a newborn are more aware of this–and worried! Newborn babies can’t tell you what’s wrong with them, so the guessing game is nonstop, and the more you see your baby in distress, the more your worry skyrockets. Although parental anxiety may suspect the worst case scenario, sneezing and a runny nose, red eyes and itchiness could also just be signs of your baby experiencing allergies.
We all know babies are fragile, and none other than parents of a newborn are more aware of this–and worried! Newborn babies can’t tell you what’s wrong with them, so the guessing game is nonstop, and the more you see your baby in distress, the more your worry skyrockets. Although parental anxiety may suspect the worst case scenario, sneezing and a runny nose, red eyes and itchiness could also just be signs of your baby experiencing allergies.
Environmental and Seasonal Allergies
In fact, even very young kids can be allergic to pollen, dust, pet dander, and mold. Babies are more likely to experience allergies to foods and eczema–especially if you have a family history of those, as well as asthma. No region is safe from allergy triggers, but if you live in nature, are in close proximity to more allergens, have indoor pets, and generally enjoy the outdoors your baby may be exposed to more allergens. If they do have seasonal allergies, then the symptoms will begin.
- Itchiness and tendency to rub the eyes, ears and nose, as well as puffy or watery eyes
- Sneezing, wheezing, and frequent mouth breathing
- Dry cough with clear mucus, and possible shortness of breath
- Irritability or excessive fatigue
Food and Medicine Allergies
Food and medicine allergies have different symptoms, which are usually seen immediately after consumption of the offensive food or medication, within a few minutes or an hour or two later at most. If your baby is allergic to medication and their reaction is hives or a rash, that may take a few days to develop. However, immediate reactions may include hives, itching, shortness of breath, vomiting, nausea, or abdominal pain. Good news is that even if other symptoms are present, anaphylaxis is rare in babies.
Treating Allergies in Babies
Even though as adults we’d rush to take an antihistamine for our allergies, this is not recommended for babies under the age of 2. The safest treatment is to reduce your baby’s exposure to the allergen: if it’s pet dander you may want to limit the time spent with pets and close off certain areas in the house; for environmental allergies you may have to keep your windows closed and invest in an air purifier; food allergies will mean eliminating the foods with allergens and possibly consider w hether allergens may transfer to your baby through breastfeeding. You should consult with your pediatrician before administering any medication, even topical skin medications such as hydrocortisone cream.
Diagnosis
The good news is that even though your baby may not be able to articulate what’s going on, your pediatrician can perform a skin test to determine possible allergies– a test usually safe on anyone over 6 months of age. A blood test could also be done for younger babies, though it is not as sensitive as a skin test. Food allergens are usually determined by process of elimination, which can be a long process as you take out the allergens from your baby’s diet one by one every week. However, at the very least when you see a difference you will know what not to feed your baby!
More
By Iris Farrou
17 Oct, 2023
Diet & Exercise, Lifestyle Tips, Prevention, Procedures, Women's Health
Bone Density, Bone Mass, DEXA, does calcium prevent osteoporosis, How to prevent onset of osteoporosis, Mineral Density, Osteoporosis, Prevention, Scan, Test, what is a DEXA scan, X-Ray
 If you have a family history of osteoporosis or are postmenopausal and suspect osteoporosis will affect your quality of life, then it may be time to take a closer look at what this “silent disease” i, how you can prevent it from taking control of your life, and the medical technology available to help you know your body.
If you have a family history of osteoporosis or are postmenopausal and suspect osteoporosis will affect your quality of life, then it may be time to take a closer look at what this “silent disease” i, how you can prevent it from taking control of your life, and the medical technology available to help you know your body.
Very simply, osteoporosis means that your bone mass and mineral density have decreased, thus diminishing the strength of your bones and increasing the risk of fractures. Although many believe only women are at risk for osteoporosis, that is not true: this disease affects men as well, and all genders as we get older. The first step to determining whether you have osteoporosis is a physical exam:
- Loss of height and weight may be signs of osteoporosis, as well as changes in posture
- If you’ve had a fracture that has not healed this is also a big sign of osteoporosis
- Balance and the way you walk can be affected by osteoporosis too
If the physical exam, along with your medical history and age, determines you may have osteoporosis then your doctor will order an exam to measure your bone density. This is where DEXA tests come in, which measure the mineral content of your bones, focusing on certain areas of your skeleton. DEXA stands for “dual-energy X-ray absorptiometry” and it is a medical imaging test; it uses very low levels of x-ray to determine how dense your bones may be (or not be).
What does the test involve?
Although it is a test you may not want to pass, medical professionals consider DEXA scans to be one of the most effective, quick and painless, as well as useful ways to diagnose osteoporosis.
- You will lie on the special DEXA x-ray table and the technologists will help you hold the desired position by using positioning devices.
- The arm of the DEXA machine will pass over your body, and two different x-ray beams with miniscule radiation distinguish bone from other tissue.
- The scanner gathers the data and translates the bone density information into pictures and graphs.
- A radiologist or other physician that has been trained in DEXA interpretation reviews and interprets the results of the scan. The expert sends a report to your primary doctor, who in turn discusses the results with you and determines the appropriate treatment.
Why is DEXA more effective than other methods?
As you may know, there are other body imaging methods that medical providers use: if you have a broken bone, you will most likely get an X-ray done, while if you experience constant headaches your doctor may order an MRI. DEXA very specifically measures bone density, and it also measures bone density in each specific area of the body. A common misconception is that our bone density is the same throughout our skeletal system, but DEXA is able to determine lean skeletal, fat, and bone masses in various spots in our body.
More
By Iris Farrou
17 Oct, 2023
Health Conditions and Pregnancy, Pregnancy, Prevention, Procedures
amnioscentesis, amniotic fluid test, fetal lung test, genetic disorders, genetic predisposition, genetic testing, gestation, Healthy pregnancy, high risk pregnancy, pregnancy health conditions, tay-sachs disease, Ultrasound
 The majority of expectant parents want to ensure their baby is as healthy as possible. Along with pre-genetic tests that determine certain genetic traits or risks parents may pass to their offspring, prenatal testings are quite common. These help you carry a healthy pregnancy to term, and check in on the baby’s health. Amniocentesis is one of these prenatal tests: it diagnoses genetic disorders and other health issues in a fetus:
The majority of expectant parents want to ensure their baby is as healthy as possible. Along with pre-genetic tests that determine certain genetic traits or risks parents may pass to their offspring, prenatal testings are quite common. These help you carry a healthy pregnancy to term, and check in on the baby’s health. Amniocentesis is one of these prenatal tests: it diagnoses genetic disorders and other health issues in a fetus:
- Fetal infection can be determined through amniocentesis, along with other illnesses
- Fetal lung testing is rarely done, but if a delivery is planned to happen sooner than 39 weeks amniotic fluid helps see if a baby’s lungs are mature enough for birth
- Sometimes there is an amniotic fluid build-up in the uterus–polyhydramnios–and it is drained through amniocentesis
What is the procedure?
It is normal to be nervous about any medical procedure, much more so if you are pregnant! The goal of amniocentesis is to extract amniotic fluid from your uterus, and most procedures happen between 15-20 weeks of gestation. Here’s what you should expect on the day of your appointment:
- You will lie on your back, just like you would prepare for a routine ultrasound. That’s the first step, as the ultrasound will show where your baby is in your uterus that particular day and time.
- The ultrasound will remain on screen as your healthcare provider inserts a very thin needle through your stomach wall and into the uterus. The needle is removed swiftly as amniotic fluid is drawn into the syringe.
- There is no sedation or numbing used, and it is important that you stay still. Even after the needle is removed, the ultrasound will remain in use to monitor your baby’s heart rate.
- You may experience mild cramping during the procedure, and/or shortly after, but you should be able to resume your normal activities after the test.
When is it necessary?
As one of many prenatal testings, amniocentesis provides details on certain genetic conditions and issues that other procedures may not fully address. It can detect chromosomal, genetic disorders, or congenital disabilities such as down syndrome, Tay-Sachs disease, neural tube defects, and Rh disease.
If the results of a routine prenatal screening test are worrisome, your doctor may suggest amniocentesis to rule out another diagnosis. If you’ve had a pregnancy with a genetic condition, amniocentesis will look for that condition in your current pregnancy. If the parents are carriers of a genetic condition, or have a family history, amniocentesis shows whether your baby is affected by it. Unusual ultrasound findings are another reason for further testing. Babies born to people over 35 have a higher risk of chromosomal conditions, so if you’ve had a prenatal cell-free DNA screening that came back positive, amniocentesis will shed light into possible conditions.
Even if your doctor suggests amniocentesis, and explains why, the final decision is up to you; as with any healthcare issue, you always have the right to seek out other professional opinions!
More
By Iris Farrou
30 Sep, 2023
Breast Cancer, Breast health, Lifestyle Tips, Prevention, Procedures, Queer Health, Women's Health
boob job, breast, breast augmentation, Breast cancer, breast lift, chest masculinization, cosmetic, gender affirming surgery, how to fix breast shape, implants, lumpectomy, male breast cancer, male breast reduction, mastectomy, men with breast cancer, partial, reconstruction, reduction, remove implants, surgery, top surgery

The conversation around breast reconstruction surgeries focuses on women who have had either a mastectomy or a lumpectomy done and wish to reconstruct their breasts once they are cancer free. This is a wonderful opportunity for women who are cancer survivors, and of course, a very body-affirming procedure as well! According to 2020 data from the American Society of Plastic Surgeons, breast augmentation surgery has been in the top 5 cosmetic surgeries since 2006, followed by breast implant removals, lifts, and reductions. The highest demographic for breast procedures are women ages 40-54. Sometimes, breast reconstruction surgeries get categorized alongside cosmetic breast procedures. Though there is definitely an overlap, these are the most common breast surgeries:
- Breast augmentation that increases the size of the breasts and may affect the shape and cleavage as well.
- Breast lift, which tightens the existing tissue for a more refined breast shape.
- A combination of breast augmentation with lift, for a one-time makeover.
- Breast revision: patients update their existing implants, can change the size or shape of their breasts, or completely remove the implants.
- Breast reduction for women with excessively large breasts that affect either their body image, create physical problems, or both.
- Male breast reduction for men with excess fat and glandular tissue on their breasts.
All of these procedures reconstruct the breasts in one way or another, and the reasons are often both cosmetic and medical, as well as mental health reasons. A prime example of this is gender affirming top surgery for trans people: either chest feminization or chest masculinization. For chest feminization, surgeons will usually recommend breast augmentation with implants or fat grafting, or a combination. When it comes to chest masculinization, surgeons perform a type of mastectomy that removes breast tissue, eliminates the crease on the bottom of the breast, and reconstructs the nipples according to the patient’s preferences.
Women who have undergone double or partial mastectomy, or a lumpectomy, may choose to have breast reconstruction surgery. Patients whose breast cancer can be removed with surgery have more options on the type of surgery they get done–and can usually have immediate reconstruction surgery right after their breast cancer surgery. However, for medical and/or personal reasons, women can also choose to have delayed reconstruction surgery: months or even years later. There are two main types of post-cancer breast reconstruction surgery:
- Flap Reconstruction: this surgery uses tissue from your own body to form one or both breasts. There are several types of flaps, and the choice is made on a case by case basis. Your surgeon will consider which type is appropriate for you, and whether you safely qualify for this type.
- Implant Reconstruction: much like the cosmetic procedure, silicone or saline implants are used to reconstruct the breast tissue. Your surgeon will either lift the chest muscle and place the implant underneath, or they may place the implant above the chest muscle if they can.
Since every body and case is different, not all options may be available. Whether for medical or cosmetic reasons, consult with your surgeon about your breast surgery options, get several opinions if you can, and see if you are eligible for insurance coverage. Keep in mind some procedures may take a long time to be completed, may need to successfully happen over a period of months, or be regularly maintained to ensure your health and safety.
More
By Iris Farrou
31 Jul, 2023
Da Vinci Robotic Surgery, Health Conditions and Pregnancy, Hysterectomy, Menopause, Peri-Menopause, Peri-Menopause, Procedures, Queer Health, Reproductive health, Robot Hysterectomy, WNY Ob-Gyn News, Women's Health
3D imaging, abnormal vaginal bleeding, Cancer Treatment, cervical, cervix, endometriosis, faster recovery, fibroids, Laparoscopic Surgery, minimally invasive surgery, Ovarian, ovaries, pelvic pain, Precancer, Robot Assisted Hysterectomy, Robot Hysterectomy, uterine, uterine prolapse, uterus
 What is it?
What is it?
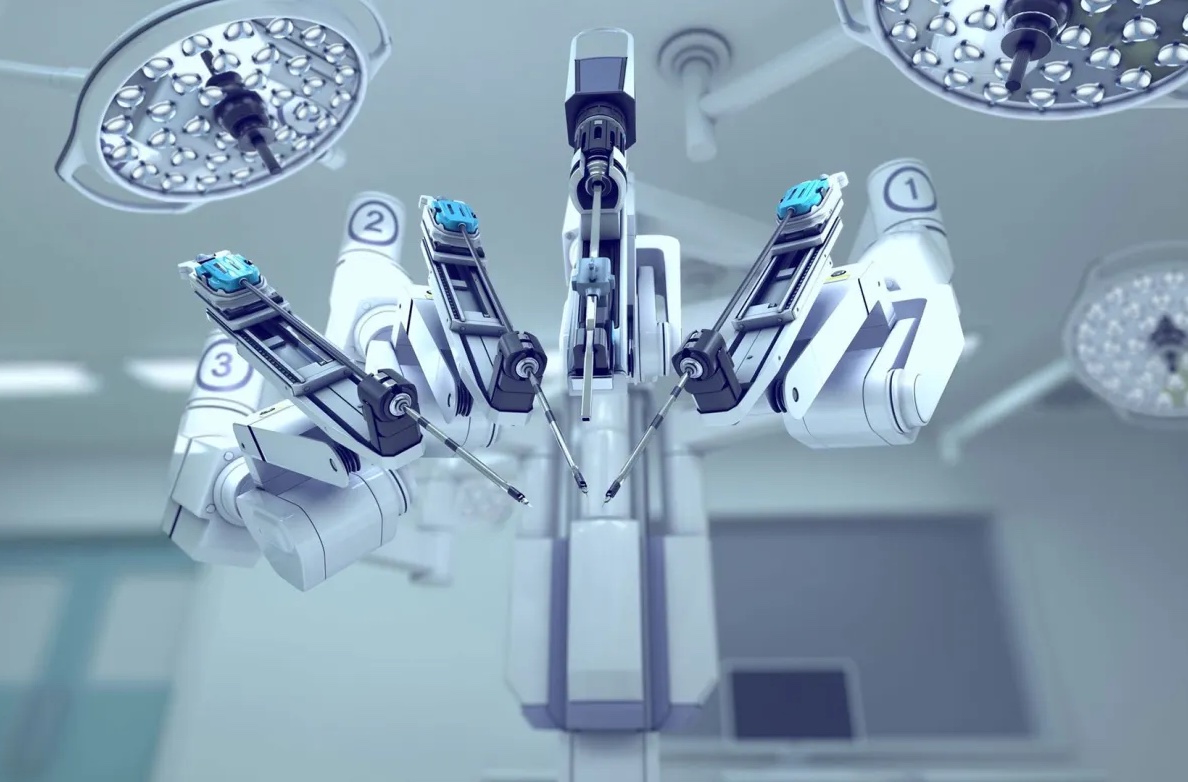
You may have heard of a traditional hysterectomy, which refers to the surgical procedure to remove the uterus (hysteros) from the body. In this case, the procedure is done with a large incision and requires longer recovery time. Nowadays, doctors can use robotic technology to their advantage–and to the advantage of the patients–to perform certain procedures, hysterectomy being one of them. In robotic hysterectomy, your doctor uses the technology to make small incisions of 1-2cm and fully controls the robotic arms with a controller while looking at a 3D magnified image of the area of surgery on their screen.
How does it work?
Robotic hysterectomy is a type of laparoscopic surgery: it is less invasive than traditional surgery, and patients experience much less pain, faster recovery, and less blood loss than open abdominal hysterectomy. Your doctor makes small incisions on your abdomen, and then inserts a laparoscope and other surgical instruments through the incisions. The laparoscope is a very thin tube with light and a camera at the end, thus projecting the surgery on a high-definition and magnified screen; this allows your surgeon to be aware of a lot more details during the surgery, as well as possible problems, than the human eye itself since the image is magnified up to 15 times.
The instruments used during robotic hysterectomy, particularly the technology of the daVinci surgical system, mimic the movement of human hands but with a lot more dexterity, precision, and flexibility. Your surgeon has full control over the instruments at all times, and they would be in the operating room just a few feet away from you. As opposed to traditional surgery where the surgeon would be standing over you for long periods of time, robotic hysterectomy allows your surgeon to utilize the constant steadiness of the robot arms to operate from angles and positions that would be typically hard to reach. Keep in mind that the robotic arms are more precise than natural hand movements, and they will not get tired during the surgery.
Who needs it?
Hysterectomies may be suggested to treat conditions like cancer or precancer of the uterus, cervix, and ovaries, uterine prolapse, endometriosis, uterine fibroids, pelvic pain, and abnormal vaginal bleeding.
Robotic hysterectomy is one of the methods surgeons can use to remove the uterus from the body, and though less invasive and more precise, surgeons decide on a case by case basis whether robotic hysterectomy is an appropriate option for their patients. Robot assisted procedures can be especially helpful if you have a complex surgical case, such as scar tissue that binds surrounding organs together and would need more precision during surgery.
What happens after it?
Like with any surgery, there will be a recovery period. Patients who have had robotic hysterectomies report that they heal faster and experience less pain; we need to remember that every body is different, and that people recover at different rates. After a robotic hysterectomy, you may be expected to stay the night at the hospital, and you may experience vaginal bleeding for a few days or weeks after your surgery. Full recovery can take 3-4 weeks, and vaginal intercourse should be avoided for at least 6 weeks after the surgery. If you are concerned about any symptoms or adverse reactions, reach out to your doctor and immediately seek professional assistance.
https://my.clevelandclinic.org/health/treatments/21057-robotic-assisted-hysterectomy
https://www.mayoclinic.org/tests-procedures/robotic-hysterectomy/about/pac-20384544
More
By Iris Farrou
14 Apr, 2023
Health Conditions and Pregnancy, Pregnancy, Procedures, Queer Health, Reproductive health, Surrogate, Women's Health
Buffalo NY, Cryogenic, Egg Freezing, Embryo Banking, Embryo Freezing, Fertility, Fertility Assistance, Fertility Preservation, Freezing My Eggs, How to save my eggs, Infertility treatment Buffalo, Oocyte Cryopreservation, Pregnancy and Infertility
Many people consider the choice of freezing their eggs so they can retrieve them at a later time and start a family. This process is, nowadays, more common than it used to be; there is more information available for people to become aware of the pros and cons, there are more facilities that can store your eggs at an affordable price, and more professionals will suggest it if you want to have your own family later in life, or are undergoing treatments that may affect your fertility.
When Should I Consider it?
Most cis-women reach the peak of their fertility at age 30. While eggs continue to be produced and can be retrieved after that age, our egg production drops significantly around age 37, and completely stops when entering menopause–usually between 45-55 years of age. Patients who are experiencing severe health concerns that may affect their fertility– such as undergoing chemotherapy, having Polycystic Ovarian Syndrome, or endometriosis– may want to consider undergoing fertility treatments and retrieve their eggs for freezing. Egg freezing is also common among individuals who are undergoing hormone replacement therapy.
What is the Process?
It is quite a straightforward process to freeze your eggs, so don’t be alarmed by the terminologies used or the clinical equipment needed. In fact, it is very similar to the process of in-vitro fertilization, with the difference being that the eggs are not fertilized immediately, but frozen. Most cycles are complete in about 2-3 weeks.
- The first step would be to meet with a fertility specialist to discuss your desire to freeze your eggs. Then, you will schedule an exam for complete medical history, bloodwork, and hormone testing. Your doctor may also recommend a transvaginal ultrasound to assess your ovarian reserve.
- You will need to monitor your menstrual cycle and determine the exact dates when you are ovulating. To get more accurate results, your doctor may recommend birth control. After that, you will start stimulating your egg production.
- Most commonly, you will start by injecting 2-3 hormone medications a day for about ten days. This will encourage a group of eggs to develop at the same time.
- To track the ovulation and development of the eggs, you will have frequent blood work done and 4-6 pelvic ultrasounds.
- Once your eggs have matured, they will be retrieved. This involves an ultrasound-guided surgical procedure that takes 20-30 minutes under anesthesia.
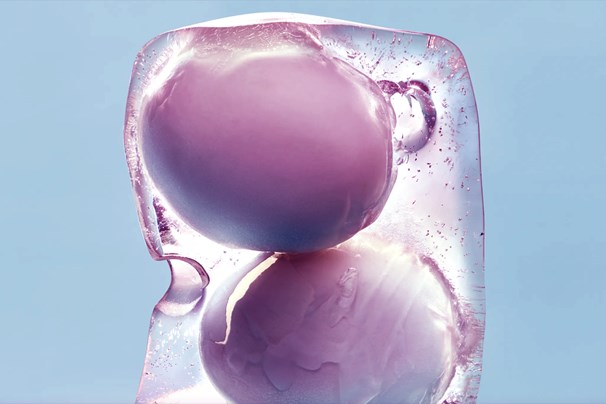
And you will have reached the final step! Once an embryologist confirms the eggs are mature, which means they will have the potential to be fertilized, your eggs will head to their deep freeze home: liquid nitrogen tanks in an embryology lab.
https://www.hopkinsmedicine.org/health/wellness-and-prevention/freezing-eggs-preserving-fertility-for-the-future
https://www.healthline.com/health/egg-freezing-process#timeline
More
By Iris Farrou
31 Mar, 2023
Fatherhood, Lifestyle Tips, New Moms, Parenting, Procedures, Your baby's health
Baby Healthcare, Infant Health, Infant Healthcare, Infant Vaccines, newborn expectations, Should I vaccinate my newborn, When should my newborn visit the doctor

If your baby is at the age when the first vaccinations are needed, it is understandable that there may be some stress surrounding the upcoming visit to the doctor. Of course, any doctor’s visit with a newborn is stressful, but it can be worse if you know there will be a needle poking your baby’s skin. Not a pretty image, but a necessary one! The first thing you can do to be adequately prepared for the situation is to educate yourself first. Read up on the first vaccines that your baby needs and the advantages that come with them; ease your mind by knowing how much safer your infant will be. You may find an easily accessible vaccine schedule from birth to 18 years at the Center for Disease Control.
Once you are more informed about the first vaccines your baby will be receiving, you can start preparing for the visit. A lot of nurses report that the number one factor that makes these first vaccinations difficult is the stress of the parents. It is important for your baby, and for the medical professionals, that you remain calm and as stress free as possible. If your baby feels you are calm, hears a soothing tone of voice from you, and picks up on reassuring messages, the calmer they will be and the easier the process will be.
To prepare for the visit, you can have a talk with your child about what will happen. You can use simple words, or imitate the motions that the doctor will perform to help them understand. Remain relaxed and upbeat while you are explaining this, and during the vaccination. Heading to the doctor’s office, you may want to bring your child’s favorite toys with you, or other items that give them comfort. That way, they will be able to focus on something pleasant.
If you are breastfeeding, it is a good idea to breastfeed right before your baby receives the vaccine. Breastfeeding is a great way to provide comforting close contact and help relax your child. You can also ask your doctor to give your baby something sweet two minutes before the shot: a small amount of sweetness can help reduce the pain of the shot. Another possibility is to ask for a pain relieving ointment or spray. This can be one your doctor provides you with and you apply before the visit, or a topical cooling spray that they will apply before the shot. Both options topically block the pain signals from the skin. Right before the shot, try to distract your child by pulling their attention away from the doctor; it can be as simple as calling their name, singing their favorite song, or telling a story. Keep the distraction going even after the vaccine is given.
After the shot is given, comfort your child by holding them close, or swaddling them. Close contact, whispers, and cuddles are all helping reduce the stress and distract from the pain. If your child has mild reactions from the shot, like topical swelling or a mild fever, don’t be alarmed as these are normal reactions. If something concerns you, however, always contact your doctor and seek further medical advice and help.
More
By Iris Farrou
28 Feb, 2023
Lifestyle Tips, PMS, Prevention, Procedures, Queer Health, Reproductive health, Sexual health, Women's Health
cysts, Fibroid Cluster, Heavy Periods, Infertility help, MRI, Ovarian, Reproductive system disorders, Symptoms, Ultrasound, Uterine Cancer, Uterine Fibroids, Womens Reproductive Health

If you have a uterus, then you already know there are countless issues to keep in mind and a full maintenance schedule for your uterine health. There is yet another concept to add to your list: uterine fibroids. Ideally, your OBGYN or primary care doctor has already talked to you about these. But if this is the first time you come across this term, fear not–uterine fibroids are extremely common, and 99% of the time they are also harmless. However, that does not mean you should ignore them, or that they don’t contribute their fair share of challenges in your cycle.
What are uterine fibroids and how do I know I have them?
Uterine fibroids, also known as leiomyomas, are quite simple: they are noncancerous growths (or tumors, though that word is admittedly scary) made up of the connective tissue and muscle from the wall of the uterus. They can grow solo, or in a cluster, and are most commonly less than 8 inches in diameter– though they can grow larger. Many people with a uterus do not even realize they have uterine fibroids, unless some of the symptoms start becoming more prominent, or you specifically ask your OBGYN to look for them.
The most common signs of uterine fibroids include heavy menstrual bleeding, periods lasting more than a week, bleeding between your periods, frequent urination or difficulty emptying your bladder–usually resulting in a feeling of heaviness in your lower abdomen–constipation, lower back pain, and even pain during sex. These symptoms are definitely not an exclusive list, and presence of such symptoms does not guarantee the only issue is uterine fibroids: if you have concerns, it is advised that you consult with your doctor so you can know exactly what you are dealing with.
How are they diagnosed and treated?
If you are concerned about the presence of uterine fibroids, you can ask to have an ultrasound done to determine the presence of uterine fibroids. The ultrasound can be transabdominal, and/or be done inside your vagina to get pictures of the uterus. Your doctor may also order blood count tests to determine if you have anemia from chronic blood loss, and to rule out other bleeding disorders. If these methods do not yield satisfactory results, there are more in depth tests that your OBGYN can order, such as an MRI, hysterosonography, or hysteroscopy.
Since uterine fibroids are benign, the recommended treatment–as long as they are not causing significant issues in your day to day life and do not interfere with your fertility–is to keep an eye on them. They rarely grow and do not tend to interfere with fertility and/or pregnancy, and also tend to shrink after menopause. There are possible medications that your doctor may prescribe, medication which control your hormone levels to create menopause-like conditions. This tricks the fibroids into thinking your body has entered menopause, and causes them to shrink along with their unpleasant effects (such as heavy bleeding). Though there are procedures available as well, this is a step you would discuss at length with your doctor.
https://www.mayoclinic.org/diseases-conditions/uterine-fibroids/diagnosis-treatment/drc-20354294
https://my.clevelandclinic.org/health/diseases/9130-uterine-fibroids#diagnosis-and-tests
More
By Iris Farrou
08 Dec, 2022
Fatherhood, Heart health, Lifestyle Tips, Mental Health, New Moms, Parenting, Postpartum, Pregnancy, Procedures, Queer Health, Reproductive health, Surrogate, WNY Ob-Gyn News, Women's Health, Your baby's health

You have probably heard of couples using surrogate mothers to conceive, or carry a pregnancy to term. The term is often associated with a couple’s fertility challenges, and difficult as those may be, it doesn’t stop being a wonderful way for a couple to have a baby– the parents who initiate the process are called the “intended parents,” and the individual carrying the fetus is the “surrogate mother.” Some of the reasons parents-to-be consider surrogacy may be:
- Trouble conceiving through IVF, which may be related to infertility of unknown origin
- Medical issues that affect the uterus, or even a previous hysterectomy
- Conditions that make the pregnancy too high-risk, such as health concerns or advanced maternal age
- Queer couples
If you didn’t know it, there are two types of surrogacy: traditional one and gestational surrogacy.
Traditional Surrogacy: this is the least commonly used method of surrogacy as it comes with more legal and emotional complexities. In traditional surrogacy, the surrogate is both the egg donor and the surrogate mother. She uses her own eggs, and therefore has a genetic relationship to the baby. During this method, the surrogate is impregnated using intrauterine insemination. The doctor uses sperm provided by the intended father, transfers it into the uterus of the surrogate, and natural fertilization of the egg takes place from then on. As medical science advances, this type of surrogacy becomes increasingly less common.
Gestational Surrogacy: this is the most commonly used type of surrogacy, and there is no genetic relationship between the surrogate mother and the fetus. Instead, an embryo is inserted into the surrogate’s uterus and she carries the pregnancy to term for the intended parents. To get to that point, the intended parents provide sperm and eggs–or use either/or from a donor–fertilize them and then have them inserted into the surrogate mother’s uterus using in vitro fertilization. In this type of surrogacy, the surrogate may be also called gestational carrier.
Why this choice?
As mentioned above, there are several health reasons why intended parents may choose to find a surrogate mother. However, the decision does not have to rely on those health reasons, and it is always deeply personal and a private decision. The most common reason people choose surrogacy over adoption is that they want to have a biological connection to their child; even though familial bonds are not necessary to build a strong, happy, and healthy family, many parents do want a biological connection to their offspring.
Surrogacy offers a safe and transparent pregnancy as the intended parents are there every step of the way. The most common concern with adoption is that the future parents do not know the medical history of the birth mother, or the father. This can raise serious concerns about their future baby’s medical history, and many parents feel uneasy not knowing whether their adoptive infant may have potentially been exposed to malnourishment or toxins in-utero.
If you are considering a surrogate option for your family, consult with your family doctor first, and keep in mind you may also need to review your state’s laws around surrogacy agreements.
https://www.surrogateparenting.com/blog/what-is-a-surrogate-mother/
https://www.fertilitypreservation.org/blog/when-to-consider-surrogacy-and-how-to-choose-the-right-one
More
By Iris Farrou
07 Sep, 2022
Breast health, Breastfeeding support, Health Conditions and Pregnancy, Lifestyle Tips, Mental Health, New Moms, Prevention, Procedures, Queer Health, Reproductive health, Women's Health, Young adults & teens
BRCA Gene, Breast cancer prevention, Breast cancer screening, Breast Exam, Breast Exam Buffalo NY, Breast Exams at Home, Buffalo NY, Buffalo OB-GYN, Cancer in women, Healthy Lifestyle, Self-Exam, Self-Examination, women's health tips
It is common practice at your regular OBGYN appointment for your doctor to perform a breast
exam, by using their hands and examining the overall the look of your breasts. Though this is no
substitute for a mammogram, which adult women are advised to have done yearly, it is a useful
method to see whether there are any visible or tactile abnormalities on your breasts. In fact, 40%
of breast cancers were diagnosed because women noticed something unusual about their breasts.

Is this something I can do at home?
Absolutely—and it is a good idea to perform a self-breast examination once every month. Consider it a monthly inspection you deserve, and one that at the very least helps you learn your body better. Using your eyes and hands for this examination, you can develop your own breast awareness and be able to immediately identify changes—should there be any, fingers crossed not!
What do I do?
First and foremost, it is important to choose a time of the month when your breast will not be as tender since this can cloud the results of the inspection. Ideally, during a time when you are not menstruating or ovulating. Secondly, remember you can (and probably should) ask your doctor or nurse practitioner for a demonstration on how to do this at home.
The most effective technique is to start with a visual examination of your breasts. Stand shirtless and braless in front of the mirror, with no-shadow casting light if possible, and place your hands at your sides. Look for any changes in size, shape, possible asymmetry, dimpling, or puckering. Check to see if your nipples are inverted. Then, inspect your breasts in a similar manner but after raising your hands above your head, palms pressed together forming an A shape. You can also lift your breasts and inspect whether the ridges on the bottom are symmetrical. Should you not trust your own vision, or if you have a visual impairment, it’s a good idea to ask a partner, trusted family member or friend, to help you with this.
Is this all?
The visual inspection is the first step. Next, you want to use the pads of your three middle
fingers. If you can’t sense very well with the pads of your fingers you can use your palm or the
backs of your fingers. You can do the tactile inspection in the shower or lying down (that way,
the breast tissue spreads and it’s easier to feel).
Now, take your time, don’t rush, and establish a routine for this part. If you do it clockwise every
time, for example, and in the same order, then after a few times you will be better able to judge
any changes in the pattern of your breasts. The goal here is to feel the depths of the breast using
different levels of pressure—so you can go over the whole tissue. Closest to the skin, use light
pressure. As you go try to feel a little deeper, use medium pressure. Closest to the chest and ribs,
use firmer pressure.
Remember that you are not looking for anything in particular, you are just learning the patterns
of your breasts. So, take deep breaths, take your time, remind yourself this is being done
absolutely for preventative reasons—just like flossing!
More
 We all know babies are fragile, and none other than parents of a newborn are more aware of this–and worried! Newborn babies can’t tell you what’s wrong with them, so the guessing game is nonstop, and the more you see your baby in distress, the more your worry skyrockets. Although parental anxiety may suspect the worst case scenario, sneezing and a runny nose, red eyes and itchiness could also just be signs of your baby experiencing allergies.
We all know babies are fragile, and none other than parents of a newborn are more aware of this–and worried! Newborn babies can’t tell you what’s wrong with them, so the guessing game is nonstop, and the more you see your baby in distress, the more your worry skyrockets. Although parental anxiety may suspect the worst case scenario, sneezing and a runny nose, red eyes and itchiness could also just be signs of your baby experiencing allergies.