By Iris Farrou
24 Sep, 2023
Lifestyle Tips, Menopause, Mental Health, Peri-Menopause, Queer Health, Reproductive health, Sexual health, Women's Health
Anxiety, asexual, asexuality, assault, boyfriend, Buffalo NY, Depression, exhaustion, fear of intimacy, fiancé, girlfriend, how to be a supportive partner, how to bring up low sex drive, husband, intimacy fears, lack of intimacy, Low libido, low sex drive, medications that kill sex drive, meds, mental health interfere with sex drive, OB/GYN, OBGYN, overwhelmed, partner, PTSD, sexual trauma, talk to my doctor about low libido, what is a healthy sex life, why does my partner not want to have sex, why is my libido gone, wife

This may be a touchy subject for many women, as on the one hand a lot of us experience low sex drive, but on the other hand we don’t talk about it! The issue becomes more complicated when healthcare providers don’t even ask us about our libido, yet hypoactive sexual desire disorder (HSDD) is quite a common issue women deal with. Additionally, many psychologists, primary healthcare providers and OBGYNs are trained to care for and treat HSDD. HSDD is defined as the absence of desire for sexual activity and/or sexual fantasies– we most often just refer to it as “low libido,” and like anything else, it can have its ebbs and flows. Lack of sex drive can be frustrating in a relationship, but it is a normal thing to be experiencing, it can be traced back to causes, and it doesn’t mean that it’s permanent or that you do not love or are attracted to your partner.
What Causes It?
Especially in women, low libido can be attributed to hormonal changes or imbalances: this can be during the menstrual cycle as estrogen and progesterone levels rise and lower, during menopause when our estrogen levels dramatically drop, in the case of a total hysterectomy, during pregnancy, or if you have PCOS–just to name a few examples.
Another common reason for low libido in women are mental health issues, as well as medications. Depression and anxiety, PTSD, and past sexual trauma can negatively affect a woman’s desire for sex. Many times, the medications used to treat mental health issues can worsen an already low libido. This does not mean an important medication should be stopped, but you can–and should–bring it up with your therapist or mental healthcare professional.
Life stressors, chronic stress, and fatigue can minimize the body’s natural sexual urges. This is even more prevalent in new mothers, or families with young kids: the everyday exhaustion, lack of sleep, and constant worry simply leave no room for sexual intimacy, or desire thereof.
What Can We Do?
If one partner has low or no interest in sex while in a healthy relationship, remember it is a team effort: it is not up to the partner who has low libido to “solve” the issue and magically become better.
- The first thing to consider and talk about, even if it’s uncomfortable, is relationship issues. Your partner’s desire for sex, or how safe they feel, may be affected by something in the relationship neither of you knew was an issue until you really examined it and talked about it.
- If you and/or your partner face mental health issues, it is important to carefully consider how those may be affecting your sex life. Especially if you take any medications, look into the side effects and talk with your therapists about how they could be affecting your sex drive, and solutions to balance that out.
- Redefine intimacy in ways that work for you, and where sex is not the goal or the starting point. You may plan a romantic date, do small daily things to lessen stress, or start with small affectionate gestures to help strengthen your romantic bond.
If you feel that your lack of interest in sex is related to a more serious health issue, either physical or mental, or to a serious issue in your relationship that you have not communicated about, it may be a good idea to seek out professional help and support. HSDD is not uncommon, and many medical professionals can assist you with it; you know your body and life circumstances best, and with a bit of assistance you will be able to get to the root of the issue much more effectively.
More
By Iris Farrou
01 Sep, 2023
Lifestyle Tips, Menopause, New Moms, Peri-Menopause, Peri-Menopause, Postpartum, Prevention, Women's Health
abdominal, Childbirth, constipation, dysfunction, floor, obesity, Pain, painful sex, pelvic, Physical Therapy, pilates, Pregnancy, pregnant, PT, tailbone, weakened pelvic floor, Why is sex painful

When we hear about pelvic floor exercises, we often associate them with either older women, or pregnant women/women who have just given birth. This is a common misconception–older women and new mothers may see immediate benefits when engaging in pelvic floor PT, but everyone can benefit from it.
No matter your age or overall physical health, if you were assigned female at birth, knowledge is power when it comes to knowing what your pelvic floor looks like, and what it does:
- Imagine your pelvic floor as a hammock of support consisting of muscles, tendons, ligaments, nerves, and connective tissue. This hammock is between the tailbone and the pubic bone.
- First and foremost, your pelvic floor supports the bowels, bladder, uterus, and vagina; there are also muscular bands that pass through the pelvic floor that encircle the urethra, vagina and anus.
- All this, when it functions properly, plays a key role in bowel and bladder control. Your pelvic floor also helps you stabilize your pelvis and your spine, and assists with sexual function.
Who is at risk of Pelvic Floor Dysfunction?
Remember that the pelvic floor is mostly made up of muscles, and like any muscles in our body those–too–can weaken or suffer damage and lead to pelvic floor dysfunction. People who have experienced pregnancy, childbirth, chronic constipation, or obesity may be at higher risk as their pelvic floor has, and does, work harder to support their normal bodily functions and the bowels/bladder.
Some of the symptoms of pelvic floor dysfunction may include pain during intercourse, bladder pain, bowel or urinary incontinence, frequent urination, persisting pubic, tailbone, or lower abdominal pain, and constipation–to name a few. More serious issues may include pelvic organ prolapse: bowel prolapse, prolapsed uterus, and even endometriosis.
How can Physical Therapy Help?
Physical therapists are not just experts who help you walk better after an injury, they are medical experts in the functions of muscles, joints, and nerves, and have an in-depth and holistic understanding of human health. Just like any medical field, PTs have areas of expertise and you may want to work with someone who is trained on pelvic floor functions.
A PT will assess your whole body after consulting with you, not just the problem or painful areas. Your medical history, symptoms, and needs will of course be taken into account to create an individualized plan for your pelvic floor health. The exercises will, and should, be done with the physical therapist–unless they assign you specific exercises to do at home. Since our pelvic floor is basically holding everything in our body together, the center so to speak, don’t be surprised if some exercises are not directly working on the pelvic area; ask your PT to explain why they are assigning you an exercise, and how it will help you. Some soreness or aches are normal after your PT sessions, but this is not a “no pain, no gain” situation: at no point during PT should you feel acute pain or strain on your muscles/ligaments.
And for this subject, the saying “the sooner, the better” cannot be emphasized enough: do not wait until you’re older, pregnant, or have any painful symptoms to get started on strengthening your pelvic floor.
More
By Iris Farrou
31 Jul, 2023
Da Vinci Robotic Surgery, Health Conditions and Pregnancy, Hysterectomy, Menopause, Peri-Menopause, Peri-Menopause, Procedures, Queer Health, Reproductive health, Robot Hysterectomy, WNY Ob-Gyn News, Women's Health
3D imaging, abnormal vaginal bleeding, Cancer Treatment, cervical, cervix, endometriosis, faster recovery, fibroids, Laparoscopic Surgery, minimally invasive surgery, Ovarian, ovaries, pelvic pain, Precancer, Robot Assisted Hysterectomy, Robot Hysterectomy, uterine, uterine prolapse, uterus
 What is it?
What is it?
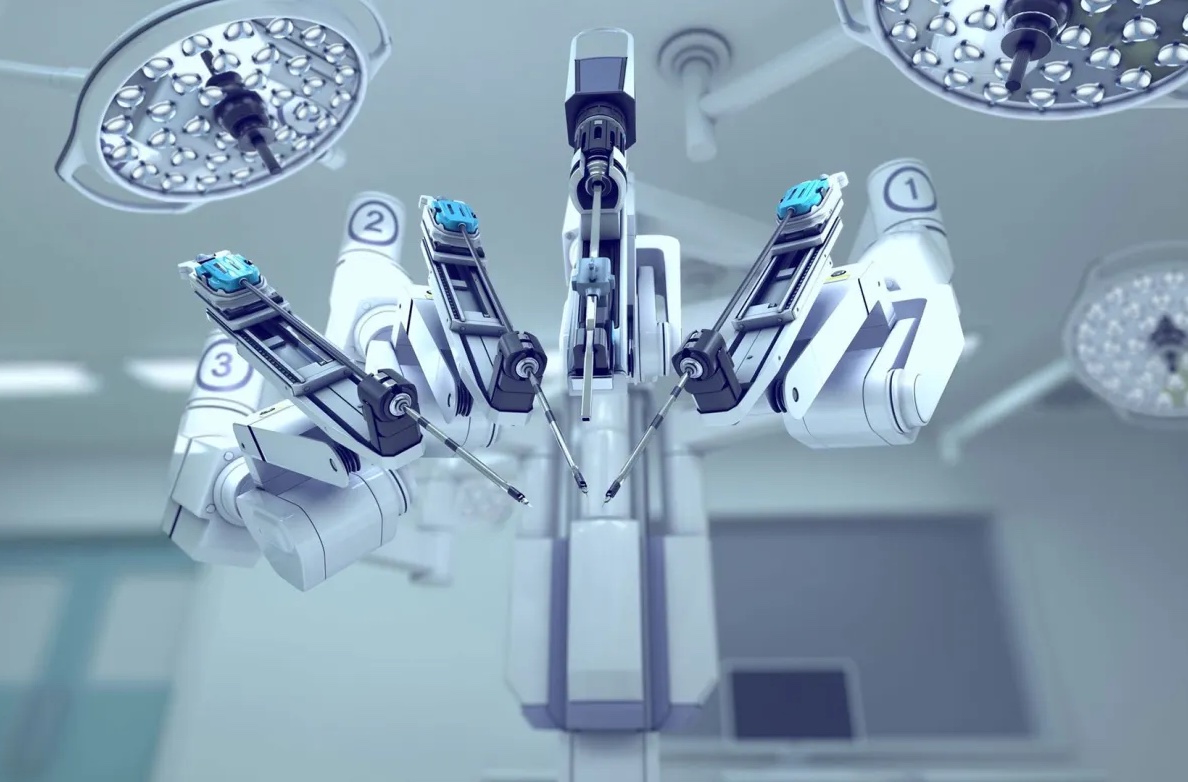
You may have heard of a traditional hysterectomy, which refers to the surgical procedure to remove the uterus (hysteros) from the body. In this case, the procedure is done with a large incision and requires longer recovery time. Nowadays, doctors can use robotic technology to their advantage–and to the advantage of the patients–to perform certain procedures, hysterectomy being one of them. In robotic hysterectomy, your doctor uses the technology to make small incisions of 1-2cm and fully controls the robotic arms with a controller while looking at a 3D magnified image of the area of surgery on their screen.
How does it work?
Robotic hysterectomy is a type of laparoscopic surgery: it is less invasive than traditional surgery, and patients experience much less pain, faster recovery, and less blood loss than open abdominal hysterectomy. Your doctor makes small incisions on your abdomen, and then inserts a laparoscope and other surgical instruments through the incisions. The laparoscope is a very thin tube with light and a camera at the end, thus projecting the surgery on a high-definition and magnified screen; this allows your surgeon to be aware of a lot more details during the surgery, as well as possible problems, than the human eye itself since the image is magnified up to 15 times.
The instruments used during robotic hysterectomy, particularly the technology of the daVinci surgical system, mimic the movement of human hands but with a lot more dexterity, precision, and flexibility. Your surgeon has full control over the instruments at all times, and they would be in the operating room just a few feet away from you. As opposed to traditional surgery where the surgeon would be standing over you for long periods of time, robotic hysterectomy allows your surgeon to utilize the constant steadiness of the robot arms to operate from angles and positions that would be typically hard to reach. Keep in mind that the robotic arms are more precise than natural hand movements, and they will not get tired during the surgery.
Who needs it?
Hysterectomies may be suggested to treat conditions like cancer or precancer of the uterus, cervix, and ovaries, uterine prolapse, endometriosis, uterine fibroids, pelvic pain, and abnormal vaginal bleeding.
Robotic hysterectomy is one of the methods surgeons can use to remove the uterus from the body, and though less invasive and more precise, surgeons decide on a case by case basis whether robotic hysterectomy is an appropriate option for their patients. Robot assisted procedures can be especially helpful if you have a complex surgical case, such as scar tissue that binds surrounding organs together and would need more precision during surgery.
What happens after it?
Like with any surgery, there will be a recovery period. Patients who have had robotic hysterectomies report that they heal faster and experience less pain; we need to remember that every body is different, and that people recover at different rates. After a robotic hysterectomy, you may be expected to stay the night at the hospital, and you may experience vaginal bleeding for a few days or weeks after your surgery. Full recovery can take 3-4 weeks, and vaginal intercourse should be avoided for at least 6 weeks after the surgery. If you are concerned about any symptoms or adverse reactions, reach out to your doctor and immediately seek professional assistance.
https://my.clevelandclinic.org/health/treatments/21057-robotic-assisted-hysterectomy
https://www.mayoclinic.org/tests-procedures/robotic-hysterectomy/about/pac-20384544
More
By Iris Farrou
22 Apr, 2023
Diet & Exercise, Lifestyle Tips, Menopause, Peri-Menopause, Peri-Menopause, Pregnancy, Prevention, Queer Health, Reproductive health, Sexual health, Women's Health
bladder control, Body Changes In Menopause, bowel function, Childbirth, core strengthening, Early menopause, ease the birthing process, estrogen loss, Frequent urination, Kegel, natural delivery, Pelvic Floor, pelvic floor dysfunction, pilates, Strengthen pelvic floor muscles, stress urinary incontinence, SUI, UTI, vaginal delivery, weak bladder

Maybe the first word that comes to mind when you hear about Pelvic Floor Exercises is “Kegel”! Yes, that’s correct– Kegel exercises are one way to exercise your pelvic floor muscles, but they are not the only ones. Kegel balls have lately become popular as an easier and faster way to strengthen your pelvic floor muscles, increase sexual pleasure, and prevent incontinence (especially if you were Assigned Female at Birth–AFAB). However, there is much debate over them, so before we worry about that we will provide some information on the benefits of pelvic floor exercises in general.
What are the benefits for AFAB people?
- Pelvic floor exercises improve bladder and bowel function control, which can be extremely helpful after childbirth or in older years. It can help with constipation, and with incontinence.
- Strong muscles on your pelvic floor can also significantly reduce the risk of prolapse.
- If you are considering childbirth, they do support vaginal delivery, and strong pelvic muscles will also greatly improve your recovery from childbirth and other gynecological surgeries.
- They are reported to help with vaginal contractions and blood flow during sex, thus increasing sexual satisfaction and orgasmic potential.
Like any self-care routine, and especially an exercise routine that helps you strengthen your muscles, training your pelvic floor muscles can help you increase your social confidence and overall quality of life.
How do they help with pregnancy and delivery?
Your pelvic floor muscles are first in line to be affected if you become pregnant; the weight of your growing baby will undeniably put extra strain on the pelvic floor. In addition to the weight, hormonal changes in pregnancy cause your muscles to soften and stretch more easily. That can lead to bladder/ bowel problems while you are pregnant and after giving birth.
It is recommended to start strengthening your pelvic floor as soon as you learn that you are pregnant. Strong muscles in the area will reduce the risk of bowel or bladder problems during your pregnancy, you will learn how to control your muscles to assist with contractions during childbirth (in the case of vaginal delivery), and with a strong pelvic floor you will return to normal much easier after delivery.
What happens to the pelvic floor after menopause?
After menopause, the production of estrogen in our bodies significantly reduces. This can lead to weaker or stiffer muscles on the pelvic floor. Connective tissues may provide less support, and along with a lifetime of bad habits and lack of specific exercise, we may be in danger of experiencing pelvic floor dysfunction.
The pelvic floor muscles are part of your spine and pelvis. If they are struggling, you may experience pain in your lower back. Weak pelvic muscles can also lead to Stress Urinary Incontinence (SUI), which means you may not be able to control your bladder during seemingly simple activities, like laughing, coughing, or sneezing. More serious pelvic dysfunctions can be pelvic organ prolapse–which can be avoided with pelvic floor rehabilitation–and bowel and urinary urgency, where we may not be able to control the urge to urinate or defecate and incidents of leakage may occur.
No matter your age, it is never too soon or too late to start looking into pelvic floor exercises or rehabilitation that are best for you, your physical condition, and your abilities.
https://www.pelvicfloorfirst.org.au/pages/pelvic-floor-muscle-exercises-for-women.html
https://www.pregnancybirthbaby.org.au/pelvic-floor-exercises
https://provenancerehab.com/aging-and-the-pelvic-floor/
More
By Iris Farrou
27 Mar, 2023
Lifestyle Tips, Menopause, Peri-Menopause, Peri-Menopause, Prevention, Queer Health, Reproductive health, Sexual health, Women's Health
Acute UTI, Aging and Painful Sex, Aging and UTIs, Am I going through menopause, Bladder Incontinence, Body Changes In Menopause, Easing the Symptoms of Menopause, Menopause, Pelvic Floor, Prevent urinary tract infection, Urinary Tract Infection, UTI

If you have a vagina, then you have possibly been warned about the dangers of Urinary Tract Infections (UTIs), and the ever-present danger that they may return and not leave you alone. Many women also report they get UTIs so often that they get used to the symptoms– so much so that they don’t realize they have an infection until it gets too bad. Because nobody likes more pain, or more health risks, let’s take a look at the three areas of the urinary tract that a UTI may affect, and the possible symptoms:
| Area |
Symptoms |
| Kidneys |
Nausea, vomiting, back/side pain, shaking and chills, high fever |
| Bladder |
Frequent and painful urination, blood in urine, pelvic pressure, lower belly discomfort |
| Urethra |
Unusual discharge, burning sensation during urination |
Did you know that UTIs are the most common bacterial infection in women over 65? Though young people certainly can suffer from a UTI, untreated UTIs in older women can lead to much more serious health issues, like kidney failure or sepsis. One reason for older women’s susceptibility to UTIs is the weakened muscles in the bladder and pelvic floor, causing incontinence or urinary retention. The longer the urine remains in the urinary tract, the higher the risk of bacterial multiplication.
Another reason why older women are at a higher risk for a UTI is because estrogen levels drop significantly after menopause. This can lead to an imbalance of good and bad bacteria in the vagina, heightening the risk of an infection. It is suggested that post menopausal women use vaginal estrogen creams, which can help support the presence of good bacteria. Drinking plenty of water and fluids, especially cranberry juice, can also help prevent infections.
No matter your age, to lessen the risk of a UTI you should also make sure you are wearing loose clothing, emptying your bladder often, wiping front to back, and always keep an eye out for possible symptoms if you have reason to be concerned. UTIs are usually treated with narrow-spectrum antibiotics, as those are more likely to be accepted by the body. In more advanced cases, UTI patients are hospitalized and receive IV antibiotics.
If you or a loved one use pads or adult diapers, you should make sure to change them often and clean the area well, pat dry, between uses. UTIs can be especially problematic for patients suffering from Alzheimer’s or dementia, as they often cannot communicate their needs or state their symptoms. In those cases, the UTI may escalate to the point where the affected person starts acting erratically, more confused than usual, and even more disoriented. If those symptoms worsen, it is definitely advisable to have elderly female patients be treated by a doctor immediately.
https://www.bannerhealth.com/healthcareblog/better-me/the-risk-of-utis-as-you-age
https://www.mayoclinic.org/diseases-conditions/urinary-tract-infection/symptoms-causes/syc-20353447
More
By Iris Farrou
05 Oct, 2022
Diet & Exercise, Lifestyle Tips, Menopause, Nutrition, Peri-Menopause, Peri-Menopause, Prevention, Queer Health, Women's Health, Young adults & teens
Bone Density, Bone Health, Calcium Deficiency, Importance of a Healthy Diet for Young Women, Nutrient Absorption, Nutrition for women, Osteoperosis, Peri-Menopause Health, Preventing Osteoporosis, Womens Nutrition

You may have heard the occasional old person complain about their bones hurting when the
weather turns, or struggle to eliminate chronic back and joint pain. Though there can be many
reasons for this, one of the most common is the silent disease of osteoporosis: it causes bones to
weaken and turn brittle and fragile. As such, the risk of broken bones or fractures is significantly
increased.
Unfortunately, if you’re not regularly tested for osteoporosis you may not even be able
to tell you have this disease until a seemingly minor accident leaves you with a broken bone…
How to Diagnose
The later stages of osteoporosis come with several symptoms, such as back pain, stooped
posture, minor fractures, and loss of height. You can, however, be proactive about osteoporosis
before you suffer those symptoms or a broken bone (seemingly out of nowhere!). The easiest
way to keep tabs on osteoporosis is a bone density test. Imagine osteoporosis turning your strong
bones into sponge-like structures. Bone density tests help compare your bone density to the
average bone density of a healthy, young, US-based woman. They are officially called Bone
Mineral Density (BMD) tests, and resemble an X-ray but with less radiation exposure. The BMD
results, along with other health factors taken into consideration, estimate your risk of having a
bone fracture in the next decade.
Getting Tested
As osteoporosis may creep up on you, it is recommended to get tested if you are a woman of
menopausal age with osteoporosis risk factors, or a woman over the age of 65. If you are under
65 but have a family history of osteoporosis and are postmenopausal, you should also get tested.
Breaking a bone after age 50 is also a good indicator you should get tested for osteoporosis.
If you have already been diagnosed with osteoporosis, and are even taking medications for it,
you may want to repeat BMD tests every couple of years. If you are switching osteoporosis
medications, it is likely that your medical professional will recommend you get tested.
Preventing Osteoporosis
There are several risk factors for osteoporosis, including age, sex, race and family history.
Women are at a greater risk for osteoporosis, as are all people as they get older. If you are white
or of Asian descent, you may also be at a higher risk. Some factors that can be controlled are low
sex hormones, excessive thyroid hormone, and other overactive parathyroid or adrenal glands.
Low calcium intake puts you at a greater risk of developing osteoporosis, as it contributes to
decreased bone density. Eating disorders or being severely underweight do the same, as they can
weaken bones in both men and women. Gastrointestinal surgery can also have a negative impact
on your bone density, as this type of surgery limits the available surface area of your body to
absorb nutrients, including calcium.
https://www.everydayhealth.com/osteoporosis/guide/symptoms/
https://www.mayoclinic.org/diseases-conditions/osteoporosis/symptoms-causes/syc-20351968
More
By Iris Farrou
07 Sep, 2022
Lifestyle Tips, Menopause, Peri-Menopause, Prevention, Queer Health, Reproductive health, Sexual health, Women's Health
Aging and Painful Sex, Body Changes In Menopause, Easing the Symptoms of Menopause, Lubricants, Lubrication, Painful Intercourse, Peri-Menopause Health, Preparing for Menopause, Sex-Positivity After Menopause, Sooth Vaginal Pain During Intercourse, treatments for vaginal dryness, Vaginal dryness
One of the most often talked about symptoms of menopause is vaginal dryness. It would be ideal if it only showed up when menopause started, but unfortunately it can start happening even a few years before menopause. Just as a bonus, women can also experience vaginal dryness after childbirth, while breast feeding, or even if they are taking certain allergy medicine or certain antidepressants.
years before menopause. Just as a bonus, women can also experience vaginal dryness after childbirth, while breast feeding, or even if they are taking certain allergy medicine or certain antidepressants.
Back to the hormonal factors, however, vaginal dryness begin hand in hand with vaginal atrophy. A truly scary word, though it simply means your body is not producing as much estrogen as before. Estrogen is responsible for the natural lubrication, elasticity, and thickness of the cervix: once estrogen production goes down, the natural lubrication of the vagina is no longer happening, and the vaginal walls can experience thinning, drying, and possible inflammations.
Lubrication
Basically, it all comes back to lubrication: since your body’s natural lubrication system retires at the age of menopause, you need to supplement vaginal lubrication via external (internal) means. Most often, especially because vaginal dryness can lead to pain during intercourse, women will turn towards vaginal lubricants. Though a great solution, it is but temporary. For something more long lasting, you may want to look into vaginal moisturizers. You can apply them every few days to moisturize and keep vaginal tissue healthy.
There is also the option to reinvigorate vaginal tissues. Science really does wonders… this can be
a low dose vaginal estrogen cream, tablet, or ring. Note that this can be prescribed in additional
to other hormonal supplements you may be taking. It is meant to specifically tackle vaginal
dryness, especially if it persists while you are on hormonal treatment post-menopause. You will
need to discuss this option with your doctors and take into consideration any other health issues
you may have faced, particularly breast cancer.
There is also the option of an oral medication, Ospemifene or Osphena, which is more geared
towards addressing vaginal pain during intercourse. It is a selective estrogen receptor modulator,
SERM, medication but women who have a high risk of breast cancer, or have faced breast
cancer, best not consider it as an option. For more details on what this medication can do for you,
consult with your doctor or medical professional.
Another technique to help you ease painful intercourse if you are post-menopausal is a nightly
vaginal suppository containing dehydroepiandrosterone (DHEA).
It’s also important to note that vaginal stimulation or even regular sexual activity, solo or with a
partner, can absolutely help post-menopausal women keep their vaginal tissues healthy. Above
all, remember this is a very natural response of your body to hormonal changes, there is nothing
to be ashamed about, and it is well within your rights to seek healthy treatments that work for
you and your body. You owe it to yourself, and though we can’t turn back the clock, we can
make sure we are living pain-free and comfortable lives within the new parameters our bodies
present to us.
More
 If you are considering feminine rejuvenation, chances are it’s vaginoplasty you have in mind. And you are correct! Vaginoplasty is the most commonly talked about type of vaginal rejuvenation, but it is not the only one. Surgical treatments include labiaplasty, clitoral hood reduction, mons pubis reduction, and vaginoplasty as part of gender affirmation surgery. There are also some non-surgical options for feminine rejuvenation treatments.
If you are considering feminine rejuvenation, chances are it’s vaginoplasty you have in mind. And you are correct! Vaginoplasty is the most commonly talked about type of vaginal rejuvenation, but it is not the only one. Surgical treatments include labiaplasty, clitoral hood reduction, mons pubis reduction, and vaginoplasty as part of gender affirmation surgery. There are also some non-surgical options for feminine rejuvenation treatments.
What Does it Do?
Overall, feminine rejuvenation treatments reshape, tighten, or reduce female genital tissues to help restore a firmer tone or symmetrical appearance. Though some patients choose feminine rejuvenation procedures for cosmetic reasons, others choose it to treat problems caused by vaginal tissue laxity, such as incontinence and discomfort during intercourse. Additionally, trans individuals who undergo gender affirmation surgery opt for vaginoplasty.
Who Needs It?
Comfort, safety, and self-confidence are major values feminine rejuvenation seeks to address. Misshapen or overly large labia can cause a lot of discomfort when exercising or wearing tighter clothing. Urinary leakage, vaginal dryness, and painful sexual intercourse are issues women face after childbirth or menopause.
The appropriate procedure can help reduce or eliminate urinary incontinence, alleviate vaginal dryness, help clothing fit more comfortably, improve sexual sensation, and provide changes to the genital area. All in all, the end goal of feminine rejuvenation methods is to alleviate any medical issues and ensure individuals are comfortable in, and happy with, their bodies.
Different Procedures
Labiaplasty: a surgical procedure to treat overly large or misshapen labia, as well as moderate to severe sagging in labial tissues, and other serious cosmetic issues that bother a patient. Discomfort is mild and recovery is fairly straightforward.
Vaginoplasty: a surgical procedure that takes place as either part of gender affirmation surgery or to treat childbirth injuries. May include different types of postsurgical care and recovery can take weeks or months.
Clitoral Hood Reduction: enlarged clitoral hoods can cause a lot of discomfort. This procedure removes excess tissue over the clitoris to address that, as well as improve sexual experiences.
Mons Pubis Reduction: for a more streamlined appearance to the pelvic area, excess fat and skin are removed from the mons pubis.
Non-Surgical Methods: most often using vaginal rejuvenation devices that emit gentle radio frequencies or therapeutic heat, non-surgical methods can help with urinary incontinence, sexual comfort, and vaginal dryness. Though the results may show quickly, they are not long lasting.
Risks
The type of feminine rejuvenation a patient undergoes depends on their unique medical condition, as well as the effect they desire to achieve. Different types of vaginal rejuvenation come with different timelines for healing, and some recoveries may be more complicated than others—vaginoplasty, for example, can take longer to heal than labiaplasty and can cause more complications during the recovery period.
If you are experiencing discomfort or are having symptoms that indicate feminine rejuvenation may help you live a healthier life, contact your medical professional to initiate an assessment and become further educated on the risks, benefits, and postsurgical care requirements associated with your case.
More
 Hormone replacement therapy (HRT) refers to any medication that contains female hormones. Women who are assigned female at birth (ciswomen) usually take it during menopause to replace the estrogen that their body stops making at this time. However, transwomen also take hormone replacement therapy to induce physical change caused by female hormones and promote the matching between gender identity and physical characteristics. Whether belonging in the former or the latter category brought you here, this piece informs you on both!
Hormone replacement therapy (HRT) refers to any medication that contains female hormones. Women who are assigned female at birth (ciswomen) usually take it during menopause to replace the estrogen that their body stops making at this time. However, transwomen also take hormone replacement therapy to induce physical change caused by female hormones and promote the matching between gender identity and physical characteristics. Whether belonging in the former or the latter category brought you here, this piece informs you on both!
Replacing Estrogen After Menopause
Two main types of estrogen therapy are given to ciswomen after menopause: systemic hormone therapy with a higher dose of estrogen that is absorbed through the body in the form of pills or cream, and low-dose vaginal products (cream or tablets) that minimize the amount of estrogen absorbed by the body. The second type is mainly used to treat the vaginal and urinary symptoms of menopause.
Feminizing Hormone Therapy
The purpose of feminizing hormone therapy is to block the action of the hormone testosterone. Estrogen is also prescribed to reduce the production of testosterone on the body and induce development of feminine secondary sex characteristics. If it is started before the changes male puberty hormones cause, then male secondary sex characteristics can be completely avoided.
What are the Risks?
For menopausal ciswomen, HRT has been found to increase the risk of heart disease, stroke, blood clots, and breast cancer. Those risks depend on the age of the patient, as women older than 60 or those who start therapy 10 years after menopause are at greater risk. Whether estrogen is given alone or with progestin can also affect the amount of risk menopausal women may face, as does each person’s individual family health history. Risk of cancer, heart disease, stroke, blood clots, liver disease and osteoporosis are factors that help determine if HRT is appropriate.
Transwomen who opt for HRT may face issues with fertility and sexual function, among other risks, including weight gain, high blood pressure, potassium, and triglycerides, type 2 diabetes, cardiovascular disease, excessive prolactin in your blood, and increased risk of breast cancer.
Benefits of HRT
If you are experiencing symptoms of menopause, such as vaginal dryness, itching, discomfort with intercourse, and the infamous hot flashes and night sweats, chances are HRT will help you alleviate those issues. Systemic estrogen also helps with osteoporosis and can lead to less bone loss and decrease the risk of fractures. If you are experiencing early menopause or estrogen deficiency, HRT can help not only with osteoporosis, but also with reducing the risk of heart disease, stroke, dementia, and mood changes.
If you are seeking HRT as part of your gender-affirming journey, then you already know that it will lessen the burden of gender dysphoria. Setting out to achieve the desired secondary sex characteristics also greatly reduces psychological and emotional distress, leading to improved mental, social, and psychological functioning. Sexual satisfaction is also known to be a positive effect of HRT among trans individuals, as is an overall improved quality of life and self-esteem.
More
 According to the National Osteoporosis Foundation (NOF), approximately 8 million women in the United States have osteoporosis, a disease that can cause bones to break with something as unavoidable as a sneeze. All women should be aware of the bone health risks they face over age 50. As women age, and particularly during the 5 to 7 years following menopause, they can lose up to 20 percent of their bone density due to decreasing estrogen levels, making their bones more fragile, and putting them at greater risk of injury. Read on to learn about the bone health risks women face after age 50, and what you can do to protect your bones at age 50, and well into the future.
According to the National Osteoporosis Foundation (NOF), approximately 8 million women in the United States have osteoporosis, a disease that can cause bones to break with something as unavoidable as a sneeze. All women should be aware of the bone health risks they face over age 50. As women age, and particularly during the 5 to 7 years following menopause, they can lose up to 20 percent of their bone density due to decreasing estrogen levels, making their bones more fragile, and putting them at greater risk of injury. Read on to learn about the bone health risks women face after age 50, and what you can do to protect your bones at age 50, and well into the future.
Bone Health Risk Factors and Your Healthy Bone Protection Plan
It’s never too late to make the types of healthy lifestyle changes needed to protect your bone health. Follow these tips below to mitigate the chances of developing osteoporosis or other bone health issues as you age.
- Obtain a bone density test from your doctor to assess your current bone health. All women should receive a bone density test during menopause, or earlier, depending on the presence of certain health factors, to determine their risk of bone health complications.
- Consume plenty of calcium. 99 percent of the calcium your body needs is stored in your bones. Women over 50 need about 1,200 milligrams of calcium per day to maintain healthy bones.
- Consume plenty of vitamin D. Just like calcium, vitamin D is essential to maintaining healthy bones as it helps to aid in calcium absorption. Without enough vitamin D, women may lose up to 4 percent of their skeletal mass every year. To maintain healthy vitamin D levels, seek out fortified dairy products, leafy greens, and natural sunlight.
- Eat more fresh vegetables and fruits. In addition to vitamin D, fruits and vegetables offer high levels of other nutrients that are key for bone health, such as vitamin K, vitamin C, potassium, magnesium, and several B vitamins.
- Add supplements as needed. Talk to your doctor about supplementing your diet to achieve the necessary vitamins and minerals. Women ages 19 to 50 need about 1,000 milligrams of calcium and 600 international units (IUs) of vitamin D per day. After menopause, or around age 50, women need about 1,200 milligrams of calcium a day, and over age 70, women need about 800 IUs of vitamin D.
- Stay active. Throughout your life, to build and maintain healthy bones, stay active with weight-bearing exercises and activities that are conducted standing up, such as running, walking, aerobics, and dancing. At least 30 minutes of activity most days is optimal for bone health.
- Maintain a healthy weight. Women who are underweight are at a higher risk of having weaker bones, putting them at a greater risk of breakage.
- Reduce caffeine. Caffeine can cause your body to eliminate calcium more quickly. Reducing your consumption of caffeinated coffee, tea, soda, and caffeinated energy drinks, mitigates these effects.
- Quit smoking. As if you didn’t need another reason to quit smoking, tobacco use is the number one cause of bone loss and bone fractures in women over age 40.
- Moderate alcohol consumption. Women who drank alcohol heavily during their body’s formative teenage years may suffer from irreversible skeletal damage and be at a greater risk of developing osteoporosis as an adult. On the other hand, moderate alcohol consumption, such as a glass of wine per day in adulthood, may help to protect bones. In sum, if you’re going to drink alcohol, simply drink moderately and don’t overindulge—at any age.
For more information about maintaining optimal bone health, or to schedule a bone density test, talk to your doctor. He or she will help you understand your unique risk factors, and the lifestyle changes you can make now for healthier bones in your future.
Chouchani, Sayegh and Robinson MD is a top OB-Gyn practice located in Western New York. We are currently accepting new patients. Give us a call today to schedule your first visit. We look forward to meeting you.
More